













 7 / 105
7 / 105

B
ladder
exstrophy
R
ev
A
ssoc
M
ed
B
ras
2016; 62(3):197-198
197
IMAGE IN MEDICINE
Bladder exstrophy
G
ustavo
G
omes
M
endes
¹*
, J
oel
R
odrigo
B
eal
L
usa
¹
1
Degree of Specialist in Radiology and Diagnostic Imaging from Colégio Brasileiro de Radiologia e Diagnóstico por Imagem (CBR)/Associação Médica Brasileira (AMB). Full Member of the Imaging Department at Hospital
A.C. Camargo Cancer Center, São Paulo, SP, Brazil
S
ummary
Study conducted at Hospital
A.C. Camargo Cancer Center,
São Paulo, SP, Brazil
Article received:
4/6/2015
Accepted for publication:
5/4/2015
*Correspondence:
Address: Rua Professor Antônio
Prudente, 211,
Liberdade
São Paulo, SP – Brazil
Postal code: 01509-010
Phone: +55 11 2189-5000
gussmendes@hotmail.com http://dx.doi.org/10.1590/1806-9282.62.03.197Bladder exstrophy is a rare congenital anomaly resulting from failure of fusion
of the middle of the pelvis line tissues during embryogenesis. It is characterized
by malformation of the lower abdominal wall involving the genitourinary tract
and the musculoskeletal system. Its incidence is estimated at 1:30,000 to 1:50,000
live births, and it is 2 or 3 times more frequent in males. The child’s age is im-
portant and the best results are obtained when treatment is performed shortly
after birth.
Keyword:
bladder exstrophy.
C
ase
Male patient, aged eight months, referred with clinical di-
agnosis of bladder exstrophy for assessment of any associ-
ated anorectal and skeletal anomalies. According to the
caregiver, this was a term birth with prenatal examinations
performed uneventfully, and diagnosis made based on mor-
phological routine ultrasound (US) during pregnancy.
D
iscussion
Bladder exstrophy is a rare congenital anomaly resulting
from failure of fusion of the middle of the pelvis line tis-
sues during embryogenesis. It is characterized by malfor-
mation of the lower abdominal wall involving the geni-
tourinary tract and the musculoskeletal system.
Its incidence is estimated at 1:30,000 to 1:50,000 live
births, and it is two or three times more frequent in males.
In the classic bladder exstrophy, the anterior wall of the
back of the bladder is exposed, and changes such as epi-
spadias, dysplasia of the pelvic floor muscles, short penis
or clitoris bifurcated are part of the clinical picture.
The child’s age is important and the best results are
obtained when treatment is performed shortly after birth.
Most pathological changes can be prevented by early clo-
sure of bladder exstrophy.
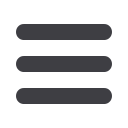
Pubic diastasis (Figures 1 and 2) is the stigma of ex-
strophy-epispadias complex malformations; it is narrow-
er in epispadias and wider in the bladder and cloacal ex-
strophy and is always associated with lateral rotation of
the femur and acetabulum. The defect of the abdominal
wall that remains after closure of the bladder is triangu-
FIGURE 1
Axial T1 magnetic resonance imaging (MRI). Diastasis
of pubic bones associated with a defect of the anterior abdominal
wall and insinuation of the anterior wall into the ventral muscles.
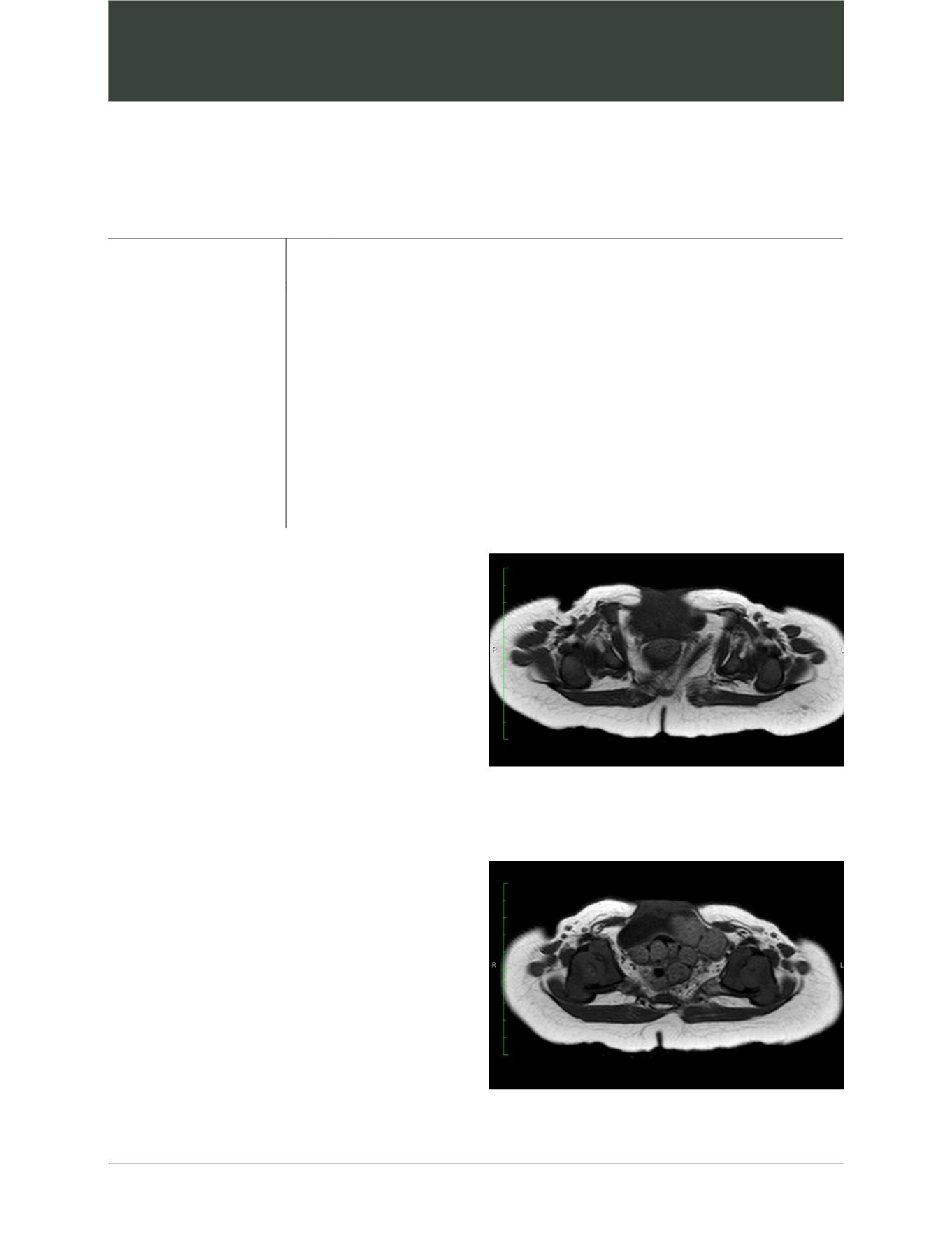
FIGURE 2
Axial T1 MRI. Insinuation of the anterior wall of the bladder
and bowel loops through lateral opening in the rectus abdominis muscle.